


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Inspiration of Foreign Bodies During Dental Practice
Ilma Robo1*, Oresto Cuni1, Andi Iseberi1, Saimir Heta2
2.Department of Pediatric Surgery, QSUT, Tirana, Albania.
Copyright : © 2018 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: In the daily practice of dental working, small instruments interferes with emergencies, if they occur, in cases where the passage of small instruments on the road of inspiration occurs.
Objective: The situation is also the cause of legal problems, so awareness of these phenomena is important.
Objectives of the study are: the road and the means necessary to prevent such urgent situations, administer these situations in our dental cabinets.
Method: Information was collected by a physician in various fields such as ORL, OMF and the dentist for such cases whether, or not, they have been administered and prevention measures. The study summarizes the presentation of a clinical case presented at the University Clinic.
Result: Case Report. The case presented in the work was monitored with radiographs until the foreign body spontaneously went off. Accidental foreign body ingestion or aspiration is usually handled by physicians in the Accident and Emergency units. A sizeable proportion of those affected are children (80%) below 3 years of age.
Conclusion: Dental and instrument materials management requires special care, especially when the patient is in an extended, or half stretched position. The dentist should be able to manage the emergency that may encounter. Preventive techniques should be used, because these incidents are preventable, if accurate precautions are taken based on legal basis. Failure to use the safety measures deemed necessary by dental science in the use of small-sized instruments constitutes negligence and is punishable by law. The dentist is obliged to limit the extent of the damages, so in the event of an incident, all necessary measures must be taken to avoid further damage, otherwise the dentist will be accused of negligence.
Keywords: foreign body, dental practice, inspiration,Dental Science
1. Introduction
Careful attention to the use of dental instruments is paramount in preventing incidents at the level of inspiration. This care needs to be increased even more in the case of children and patients with specific needs. In our daily practice, the dentists work with relatively small instruments in size. Inspiration or passage of these instruments into the respiratory tract is a medical emergency. In this paper appear the symptoms and the administration of these cases to come to some extent to help our colleagues.
1. The road and the means necessary to prevent such urgent situations.
2. Administer these situations in our dental cabinets.
3. Presentation of clinical cases.
The management of dental materials and instruments requires particular care especially if the patient is supine or semi-recumbent position. The dentist must be able to manage emergency situations in which patients accidentally inspire, or swallow dental instruments or materials, during treatment. Preventive techniques must be put in place because these incidents are preventable if the correct precautions are taken[1].
At present, no clear guidelines exist regarding prevention of this emergency in practice, bur exist some articles that show flow chart outlining management options and strategies to aid the clinician in the event of such an emergency is also presented[2]. Different article represented several institutional retrospective review of incidents involving aspiration and ingestion of dental foreign. This was undertaken to determine which dental procedures were more likely to involve aspiration or ingestion, as well as to evaluate the outcome of these adverse incidents[3].
1. Frequent touches of the sore area by the patient.
2. The faint pangs followed by cyanosis.
3. Cough
4. Ingestion, vomiting.
5. dyspnea
6. Laryngeal edema
7. Serious complications such as cardiac arrest
8. Risk of pleural and pneumothorax peripheral
1. The upper body of the patient is raised at a 20/30 angle with a supported head
2. Ask the patient if they can cough (often stuck bodies may get out of order, especially if they have not passed the epiglotis level).
3. If coughing is difficult in breathing, then the foreign body is in the larynx and the patient can no longer cough.
4. Heimlich maneuver is performed in cases where the patient is in danger of drowning that may lead to death, the foreign body can be pulled out of the throat by tightening the stomach in the direction of the diaphragm to increase the pressure in the tracheo-bronchial system.
5. Patient's hospitalization
1. Use of the rubber dam.
2. Removing broken prostheses.
3. Incorporating a steel wire into prothesis helps to stabilize the broken prosthesis and make it easier to identify x-ray.
4. Patients with swallowing problems or cough are always treated in a sitting or slightly stretched position.
2. Methodology
Information was collected by a physician in various fields such as ORL, OMF and the dentist for such cases whether, or not, they have been administered and prevention measures[3]. Various information and literature was gathered. Finding a clinical case presented in the paper.
Patients with the first letters: RH
Age: 13
Presented to the urgency of ORL with a pastel orthodontic wire in the larynx.
Performs neutralization of the patient.
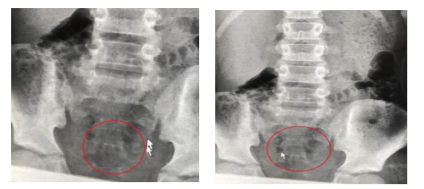
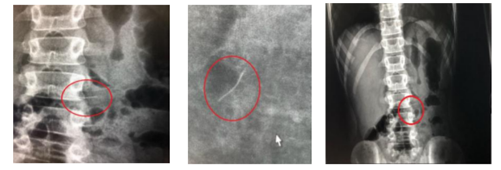
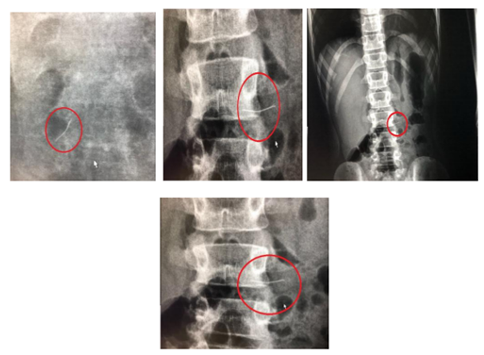
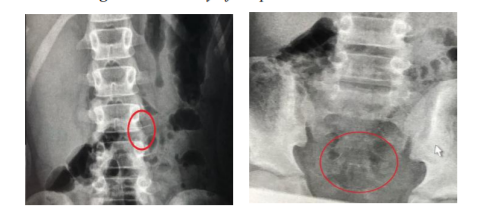
After reviewing the case, it is decided to keep the patient under x-rays several times a day.
After making 25 radiographs, the foreign body spontaneously went out.
All stages are shown in the figures 1-4, that are shown below.
3. Results
Accidental foreign body ingestion or aspiration is usually handled by physicians in the Accident and Emergency units. A sizeable proportion of those affected are children (80%) below 3 years of age[2].
While food materials constitute the majority of foreign bodies found in the airway in children [7] loose dentures, broken orthodontic appliances, or components and dental instruments are the second most commonly ingested objects in adults[3].
According to an article [3] the inspired objects may be: lower spring retainer [7] fractured twin block appliance,[8] expansion keys,[9,10] fragment of maxillary removable appliance, [11] retainer,[12] transpalatal arch,[13] and pieces of archwire[14]. A rare case of accidental swallowing of a removable quadhelix by a 13-year-old boy affected by Down’s syndrome, which necessitated surgical removal, has also been reported[15].
From this study, it is noticed that doctors in everyday practice often encounter such medical emergencies. The case presented in the work was monitored with radiographs until the foreign body spontaneously went off. The case involved in the study was one of the cases treated in the Clinic, with the fate that the dental instrument came out naturally. this case was one of many, which was attended only by radiography control. in the most complicated cases, surgical intervention for removal of dental instruments was also needed. dental instruments, however, are small, may be with or without drilling tip. Top tips are dangerous as they can spit and open complications in the event of their blockage or blockage in the affected organs rivers.
4. Conclusions
Dental and instrument materials management requires special care, especially when the patient is in an extended, or half stretched position. The dentist should be able to manage the emergency that may encounter. Preventive techniques should be used, because these incidents are preventable, if accurate precautions are taken based on legal basis. Failure to use the safety measures deemed necessary by dental science in the use of small-sized instruments constitutes negligence and is punishable by law. The dentist is obliged to limit the extent of the damages, so in the event of an incident, all necessary measures must be taken to avoid further damage, otherwise the dentist will be accused of negligence.
Acknowledgments
Our thanks belong to our family’s.
References
- Cossellu G1, Farronato G1, Carrassi A1, Angiero F2.” Accidental aspiration of foreign bodies in dental practice: clinical management and prevention”; Gerodontology. 2015 Sep;32(3):229-33. doi: 10.1111/ger. 12068. Epub 2013 Sep 19.
- Uday Kumar Umesan,1 Kui Lay Chua,1 and Priya Balakrishnan; “Prevention and management of accidental foreign body ingestion and aspiration in orthodontic practice”; Ther Clin Risk Manag. 2012; 8: 245– 252.; Published online 2012 May 23. doi: 10.2147/TCRM.S30639; PMCID: PMC33 73200; PMID: 22701326.
- Tiwana KK, Morton T, Tiwana PS. Aspiration and ingestion in dental practice: a 10-year institutional review. J Am Dent Assoc. 2004;135(9):1287–1291. [PubMed]
- Maleki M, Evans ėE (1990) External-body perforation of the intestinal tract. Report of 12 cases and review of the literature Arch Surg 101: 475-7
- Prakash UBS, Cortese DA (2004) Tracheobronchial Foreign Bodies Chapter 18, In: Prakash UBS (Ed.). Bronchoscopy. 2. Aufl. Raven Press, New York, 253 277
- Zitzmann NU, Fried R, Elsasser S, Marinello CP (2008) The aspiration and reduction of foreign bodies. The management of the aspiration or illumination of foreign bodies during dental treatment Schweiz Monatsschr Za
- Hinkle FG. Ingested retainer: a case report. Am J Orthod Dentofacial Orthop. 1987;92(1):46–49. [PubMed]
- Rohida NS, Bhad WA. Accidental ingestion of a fractured twin-block appliance. Am J Orthod Dentofacial Orthop. 2011;139(1):123–125. [PubMed]
- Nazif MM, Ready MA. Accidental swallowing of orthodontic expansion appliance keys: report of two cases. ASDC J Dent Child. 1983;50(2): 126–127. [PubMed]
- Tripathi T, Rai P, Singh H. Foreign body ingestion of orthodontic origin. Am J Orthod Dentofacial Orthop. 2011;139(2):279–283. [PubMed]
- Parkhouse RC. Medical complications in orthodontics. Br J Orthod. 1991;18(1):51–57. [PubMed]
- Klein AM, Schoem SR. Unrecognized aspiration of a dental retainer: a case report. Otolaryngol Head Neck Surg. 2002;126(4):438– 439. [PubMed]
- Abdel-Kader HM. Broken orthodontic trans-palatal archwire stuck to the throat of orthodontic patient: is it strange? J Orthod. 2003;30(1):11. [PubMed]
- Lee BW. Case report – swallowed piece of archwire. Aust Orthod J. 1992;12(3):169–170. [PubMed]
- Allwork JJ, Edwards IR, Welch IM. Ingestion of a quadhelix appliance requiring surgical removal: a case report. J Orthod. 2007;34(3): 154–157. [PubMed]