


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Emerging Concern of Cardiovascular Complications in Children with Human Immunodeficiency Virus Infection in Sub-Saharan Africa: A Systematic Review
Azene Dessie Mengistu
Copyright : © 2017 . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Sub-Saharan Africa remains to be the epicenter of the HIV-epidemic including in children. With the advent of highly active antiretroviral therapy (HAART), human immunodeficiency type 1(HIV-1) infection has become a chronic and manageable disease with longer life expectancy in the pediatric population. However, with the improved survival and decreased morbidity from opportunistic infections, HIV-associated cardiovascular complications are emerging and becoming challenging issues in routine patient management.
Objectives: The goal of this clinical review is to describe the epidemiology and clinical spectrum of HIV-associated cardiovascular diseases in children with an emphasis on Africa where it is home to the majority of the world’s HIV- infected population.
Materials and Methods: Literature search for published evidence on cardiovascular complications of HIV-infection was conducted on MEDLINE, EMBASE and Cochrane collaboration and the Cochrane Register of Controlled Trials. The following key terms were used: human immunodeficiency virus, acquired immunodeficiency syndrome, cardiomyopathy, pericardial effusion, pulmonary hypertension, infective endocarditis, rhythm abnormalities, and accelerated atherosclerosis. Additional relevant articles were retrieved from bibliographies.
Results: The spectrum of HIV- related cardiovascular complications in children and adolescents include in the form of focal myocarditis, cardiomyopathy, pericardial effusion, pulmonary hypertension, rhythm abnormalities and accelerated atherosclerosis.There is evidence from several studies that HAART has decreased overall mortality associated with HIV- infection and has a significant cardioprotective effect emphasizing the importance of universal access to HAART in HIV-infected individuals particularly in sub-Saharan Africa.
Conclusion and Recommendation: Routine evaluation of HIV –infected children is strongly suggested for potential HIV-associated cardiovascular complications in the continuum of HIV care and treatment. The occurrence of cardiac symptoms warrants a formal cardiac assessment including baseline echocardiography, electrocardiography, and Holter monitoring.
human immunodeficiency virus, children, cardiomyopathy, pericardial effusion, infective endocarditis, pulmonary hypertension, atherosclerosis, sub-Saharan Africa,AIDS
1. Introduction
Worldwide, between 34 and 41 million people was living with HIV at the end of 2014. During the same period, nearly 1.2 million people died from AIDS-related causes including cardiovascular complications. Sub-Saharan Africa remains the region most severely affected by HIV infection accounting for 66% of the globa total of new HIV infections. In 2014 alone, there were 190,000 new HIV infections among children in sub-Saharan Africa [4].Unfortunately, the incidence of AIDS-related cardiac disease is also very high in Africa compared to that seen in the developed countries[2,3,5,6].
Cardiac complications of human immunode - ficiency virus (HIV) were appreciated early in the epidemic of acquired immunodeficiency syndrome (AIDS), even before the etiologic agent, the virus itself, was isolated and characterized [1].Globally, infection with HIV is a leading cause of acquired heart disease and specifically of symptomatic heart failure, accelerated atherosclerosis and pulmonary hypertension. Human immunodeficiency virus related cardiac abnormalities tend to occur late in the disease in those with AIDS or prolonged viral infection [2,3].
Longitudinal cardiovascular studies have shown that all components of the cardiovascular system are vulnerable during the course of the disease process. The possible causes of HIV associated cardiac disease include HIV directly affecting the heart, opportunistic infections, side effects of therapy, nutritional deficiencies, or yet unknown mechanisms[7].
There is paucity of published data addressing the cardiovascular complications of pediatric HIV infection from African setting. Hence, the goal of this clinical review is to describe the clinical spectrum of HIV-associated cardiovascular diseases in children with an emphasis on sub-Saharan Africa where it is home to the majority of the world’s HIV-infected population.
2. Materials And Methods
Literature search for published evidence on cardiovascular complications of HIV-infection was conducted on MEDLINE, EMBRASE (inclusive from 1980-2015) and Cochrane collaboration and the Cochrane Register of Controlled Trials. The following search terms were used: human immunodeficiency virus, acquired immunodeficiency syndrome, cardiomyopathy, pericardial effusion, pulmonary hypertension, infective endocarditis, rhythm abnormalities, and accelerated atherosclerosis. Additional relevant articles were retrieved from bibliographies. Articles in both full text and abstract form were included.
As to eligibility criteria randomized clinical trials, observational cohort studies (retrospective and prospective), case control studies and case reports that had been published in English language were included. The selected outcome measures were potential cardiovascular compl - ications of HIV infection: cardiomyopa -thy, pericardial effusion, infective endocarditis, pulmonary hypertension, rhythm abnormalities and accelerated atherosclerosis.
The studies were assessed for use of an appropriate source population, measurement methods of exposure and outcome, methods to deal with design specific issues such as bias and lost to follow up. Data extraction and synthesis was done using a prepared data extraction sheet for the specific HIV-associated cardiovascular complications.
3. Results
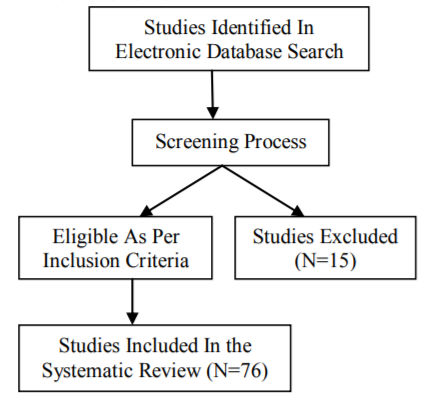
A total of ninety one studies were identified through electronic database searching. After adjusting for duplicates eighty four remained. Of these eight studies were discarded because after reviewing the abstracts it was found that these papers did not fulfil the inclusion criteria or full text of the study was not available in English language.
It appeared that fifteen studies did not meet the eligibility criteria as described in the flow diagram (Fig.1).The rest of the relevant papers met the inclusion criteria and were included in the systematic review.
4. Discussion
Most of the published data about cardiovascular complications of HIV/AIDS have been in adults. However, HIV-related cardiac complications in children are very similar to the spectrum of disease described in adults with few exceptions [8].In developed countries, antiretroviral therapy has transformed HIV/AIDS in to a chronic and manageable condition in HIV- infected children. On the other hand, the spectrum of HIV related concerns has shifted from reduction of mortality towards long-term complications of HIV disease including various HIV- associated cardiovascular complications.
Human immunodeficiency virus- associated myocardial disease might be in the form of myocarditis or cardiomyopathy with systolic or diastolic dysfunction[3,8,9].One longitudinal study revealed that among HIV-infected children up to 10 years old in the pre-HAART era,25% died of chronic cardiac disease and 28% experienced serious cardiac events after an AIDS – defining illness[10].In low and middle income countries, HIV associated cardio - myopathy is a commonly encountered HIV-associated cardiac disease[5,11-13].
A multinational prospective registry of acute heart failure in sub-Saharan Africa showed that HIV-related cardiomyopathy is one of the causes of heart failure in the region [14].Few studies in Africa and the Indian sub-continent, also demonstrated that HIV-associated myocardial disease is a commonly encountered clinical problem in this patient population [6,15-17,18,20].A multicenter, observational, prospective cohort study among ART naïve patients showed that HIV-associated cardiomyo -pathy is a significant clinical problem in HIV-infected patients not receiving HAART. In the same study, it was reported that low socioeconomic status, CD4 count, HIV1-viral load, disease stage and low serum selenium level were significantly associated risk factors for HIV-associated myocardial disease[15]. Nzuobontane et al from Yaoude, Cameroon, also reported that dilated cardiomyopathy occurred in nearly a quarter of HIV-infected ART naïve patients and it was found to be associated with low CD4 count [18].
However, a study among HIV-infected Thai children failed to show the correlation between left ventricular dysfunction and HIV disease stage and nutritional status [19].Such inconsistent research work reports might be partly explained by the difference in the study population and the difference in the ART status. Because ART has significant effects on the risk factors of HIV- associated cardiovascular disease in children [21].
Several studies described that the factors that contribute to the development of myocardial dysfunction in HIV- infected individuals are multifactorial which include cytokine dysregulation, selenium deficiency, autoimmune reaction, and cardiotoxicity from therapeutic agents [22-24]. In one study, a significant selenium deficiency was demonstrated in AIDS patients [25].There is also evidence that cardiomyopathy was reversed by selenium supplementation in HIV-infected pediatric patient [23].Because nutritional deficiencies are quite common in HIV- infected children in sub-Saharan Africa, nutritional supplementation might be of help in mitigating malnutrition associated cardiomyopathy in this patient population.
Animal studies showed that cardiotoxicity from therapeutic agents such as pentamidine and possibly zidovudine produces cardiomyopathy in mice with pathologic changes in the mitochodraia[26]. A prospective, echocardiographic study with a review of clinical records and laboratory data was reported in 137 HIV-infected children receiving zidovudine, didanosine, both or no antiretroviraltherapy. In this study, the odds that dilated cardiomyopathy would develop was 8.4 times greater in children who had previously received zidovudine than those who had not [27].
An African follow up study from Kinshasa, Congo demonstrated that more than half of HIV- infected patients develop cardiac lesions. In a similar study, low socioeconomic status which is undoubtedly a common scenario in most African countries was reported to be one of the independent predictors of mortality [28].In children left ventricular fractional shortening was found to be a useful predictor of mortality, and left ventricular wall thickness a useful short-term predictor [10,29].A prospective cohort study also showed that over a 2 year period approximately 10% of HIV – infected children had congestive heart failure[30].
On the other hand, several studies showed that HAART decreased overall mortality associated with HIV infection and it has significant cardioprotective benefit by significantly decreasing the incidence of cadiomyopathy among HIV-infected children[31-33,35-37].In the largest study to date of pediatric patients, over 3000 children with HIV-infection were longitudinally followed for incident cardiomyopathy and assess the effect of HAART. In this study, the authors noted that the incidence of cardiomyopathy decreased dramatically in the post-HAART era from 25.6 cases per 1000 person-years to 3.9 cases per 100 person-years(34). However, patients remain at increased risk of cardiomyopathy if there is ongoing exposure to zidovudine [27,34].
Hence, universal access to HAART appears to be a good strategy to decrease HIV-related heart disease in developing countries particularly in sub-Saharan Africa.
Several studies revealed that pericardial disease is commonly observed in patients with HIV infection[7,38-41].Before the HAART era, pericardial effusion occurred in up to 11% of patients with AIDS[42].According to one report the prevalence of pericardial effusion in pediatric patients with AIDS is quite high(68%) and is often associated with other HIV associated cardiac disease[38].However, a prospective and multicenter cohort study in a developed country setting showed that pericardial effusion in HIV infected patients is less frequent in the era of HAART compared to the pre-HAART period emphasizing the role of antiretroviral therapy in reducing the burden of HIV-associated pericardial disease[42].
On the other hand, in sub-Saharan Africa, the incidence of AIDS-related pericardial disease is very high compared to that seen in western developed countries [7]. Cegielski and colleagues from Tanzania reported that pericardial effusion is strongly associated with an early manifestation of HIV infection(43).
The clinical spectrum of disease etiology in HIV infected patients with pericardial effusions is associated with opportunistic infection or malignancy particularly lymphoma and Kaposi’s sarcoma. In a review of 74 reported cases of cardiac tamponade in HIV infected patients, the major causes were idiopathic(45%),mycobateria(20%),bacteria(19 %),lymphoma(7%),Kaposi’s sarcoma(5%),viruses(3%) and fungi(1%)[44].Hence, more than half of symptomatic patients with HIV- associated pericarditis have an identifiable ,and possibly treatable etiology.
In sub-Saharan Africa, where tuberculosis is endemic and access to ART is limited, pericardial disease is one of the most common forms of heart disease seen in HIV infected patients [2,5,44,46].Tuberculouspericarditis is the most common cause of pericarditis in Africa and studies from Malawi and other African country demonstrated that tuberculous pericardial effusion is strongly associated with HIV infection [43,45,46]. Although HIV-related pericardial effusion is in the majority of patients small and asymptomatic, it is a bad prognostic sign. However, the pericardial effusions rarely directly contribute to mortality but rather serve as a marker of advanced HIV infection [23,42].
Pulmonary arterial hypertension(PAH) is a progressive disease characterized by elevated pulmonary arterial pressure and pulmonary vascular resistance(PVR) leading to right ventricular failure and premature death[32,47,51].Human immunodeficiency virus-related PAH is a rare entity with an estimated prevalence of 0.5% in HIV- infected patients. This rate is, however, 25-fold higher than the prevalence of PAH in the general population [47,48].
There is paucity of published data about the prevalence of HIV-related PAH in Sub-Saharan Africa. Few available studies based on echocardiography suggested that PAH were found in the range of 0.6-15% of HIV-infected individuals which is notably high compared with to those in developed countries [39,49,50].Although interstitial lung disease and vascular bed destruction by multiple pulmonary infections were thought to be involved in the pathogenesis, the exact mechanism by which idiopathic pulmonary hypertension might occur in HIV- infected patients is not well understood.One study suggested that HIV may cause endothelial damage and mediator-related vasoconstriction through stimulation by the envelope gp120,including direct release and effects of endothelin-1(vasoconstrictor),interleukin-6 and TNF-α in the pulmonary arteries.Unlike HIV-associated dilated cardiomyopathy, there was no relationship identified in the published data between CD4 cell count and HIV-related PAH[47].
Studies showed that the prevalence of HIV– related PAH has remained at 0.5% even in the modern era of HIV therapy, suggesting that HAART has not made a dramatic impact on its prevention and why HAART has not reduced the incidence or course of PAH is unknown .In view of its poor outcome once it occurs in HIV –infected patients, routine clinical and echocardiography evaluation is suggested for early detection and aggressive treatment in this patient population.
Most of the studies on infective endocarditis in HIV- infected individuals had been in adults. Although infective endocarditis had been reported in the literature as the first presentation of AIDS in an infant, it is rarely reported in pediatric patients [52].Common organisms reported to be associated with endocarditis in HIV include Staphylococcus aureus and Salmonella species . Nel SH et al reported no significant differences in the clinical presentation of infective endocarditis between HIV-infected and HIV-negative patients [54].
One retrospective study demonstrated that the incidence of infective endocarditis has declined with the introduction of HAART. In the same study, it was also shown that increased risk of infective endocarditis was associated with low CD4 count(< 50cells/microL) and high viral load (>100,000 copies/ml) and a history of intravenous drug abuse [55].The treatment approach to infective endocarditis in HIV-infected patients is similar to the approach to those who are HIV-seronegative.In 105 HIV- infected patients with infective endoc - arditis, severe immuno suppression and left side valvular involvement were associated with greater risk for mortality[53].
Various conduction system abnormalities have been described in patients with HIV infection. In a prospective series of 31 pediatric patients with AIDS, the occurrence of frequent rhythm abnormalities was reported[56].According to one autopsy study in six children who died of AIDS the identified histological abnormalities in the conduction system were vasculitis, myocard -itis and fragmentation with lobulation and fibrosis of the conduction system[57].
A cross-sectional study from Nigerria found that the QTc interval and resting heart rate were higher in ART naïve HIV infected patients suggesting that such patients are at a higher risk of sudden death [59].A research work from a developing country setting also demonstrated that sudden cardiac deaths account for most cardiac and non-AIDS natural deaths in HIV-infected patients .There is also a published data evidence that infection with HIV is independently associated with QTc prolongation which is almost doubled with hepatitis C co-infection and associated with a 4.5 fold higher than expected rate of sudden death[60].
Patients with HIV infection are at increased risk of developing coronary heart disease at a younger age without traditional risk factors .Studies showed that endothelial dysfunction is the most plausible link between HIV infection and atherosclerosis. Increased expression of adhesion molecules, such as intercellular adhesion molecule (ICAM-1) and endothelial adhesion molecule (E-selectin), and inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin (IL-6) occur in HIV-positive patients contributing the development of accelerated atherosclerosis [61].
The long-term benefits of ART are associated with metabolic complications including lipodystrophy, dyslipidemias, lactic acidosis, glucose intolerance, osteopenia and osteoporosis [63]. According to one study, the prevalence of lipodystrophy ranges from 1 to 57% among HIV infected children and from 2 to 84% among HIV- infected adults . In a large prospective study, it was also demonstrated the occurrences of fat redistribution being observed in 42% of children after more than 5 years of ART suggesting that such metabolic complication of ART remain a serious and on-going problem in perinatally HIV- infected children[62].
Protease inhibitors(PI) have consistently been associated with dyslipidemias(increased cholesterol and triglycerides) in children which may increase the risk of accelerated atherosclerosis in early adulthood[63].The cardio-metabolic effects of protease inhibitors was also described in animal studies showing increased LDL-cholesterol[64].On the other hand, a randomized trial among HIV- infected individuals on HAART,showed that low cholesterol diet reduces the incidence of dyslipidemia emphasizing the importance of dietary adjustments while being on antiretroviral therapy[65].
In view of the published evidences that chronic HIV therapy is associated with the development of several metabolic disturbances particularly dyslipidemia,it is recommended to obtain lipid profiles from all HIV-infected children prior to the initiation of ART with subsequent monitoring every 6 to 12 months once they are on HAART[63].
5. Conclusion And Recommendation
Antiretroviral therapy made the long-term outcome of perinatally infected children with HIV-1 encouraging. However, with longer survival, its clinical sequelae are changing and HIV associated cardiovascular complications are one of the emerging and challenging issues in the continuum of HIV care and treatment articularly in adolescents[66-68].Higher prevalence of HIV –related cardiac complications tend to occur among children with most advanced clinical and immunologic category of HIV disease.Predictors of serious cardiac events include recurrent bacterial infection,wasting,encephalopathy,male gender,lower CD4 and IgG levels and earlier year of AIDS diagnosis[69].
There is evidence suggesting that in low and middle-income countries, chronic cardiovascular diseases are increasing in HIV-infected individuals [72].In sub-Saharan Africa little is known about the knowledge and practice of HIV-infected patients about the potential cardiovascular complications. A cross-sectional study from Kenya revealed that adult patients living with HIV lack the knowledge that they are at risk of cardiac complications [70].
As part of the continuum of pediatric HIV care and treatment, systematic cardiac evaluation including a comprehensive history and cardiac examination are essential for HIV- infected patients.It is prudent to be aware that cardiac symptoms, when present, are disguised by secondary effects of HIV-infection. However, the occurrence of cardiac symptoms warrants a formal cardiac assessment including baseline echocardiography, electrocardiography, and Holter monitoring preferably by a cardiologist. Studies in resource rich setting suggest that routine screening of HIV-infected individuals for associated cardiovascular diseases with involvement of cardiologists could be economically attractive [72-76].However; there is no evidence for the feasibility of routine HIV-related cardiac disease screening in sub-Saharan Africa which is the epicenter of the pandemic.
Based on the available evidence, strategic preventive interventions to mitigate the burden of HIV- associated cardiovascular complications include timely initiation of HAART as per local guidelines with appropriate monitoring, low cholesterol diet and exercise 65],71, 73].Considering the proven cardioprotective benefit of HAART, universal access to antiretroviral therapy is strongly recommended particularly in sub-Saharan Africa where the majority of HIV infected individuals reside.
6. Acknowledgment
I would like to thank Children’s Heart Fund of Ethiopia (CHFE) for supporting the review research work.
References
- Sani MU. Myocardial disease in human immunodeficiency virus (HIV) infection: a review. Wien Klin Wochenschr 2008; 120:77
- NtsekheM,Hakim J. Impact of Human ImmunodeficiencyVirus Infection on cardiovascular disease in Africa. Circulation 2005;112:3602-3607
- Magula NP, Mayosi BM.Cardiac involvement in HIV-infected people living in Africa: a review.Cardiovasc J south Afr 2003;14:231-237
- Joint United Nations Program on HIV/AIDS.UNAIDS 2014 report on the global AIDS epidemic. Available at: http://www.unaids.org/.
- NtsekheM,MyosiBM. Cardiac manifestations of HIV infection: an African perspective.Nat Clin Pract Cardiovas Med 2009;6(2):120-7
- LubegaS, Zirembuzi GW. Heart disease among children with HIV/AIDS attending the paediatric infectous disease clinic at Mulago Hospital. African Health Sciences 2005; 5(3):219-226.
- Gopal M, Bhaskaran A, Khalif WI et al. Heart disease in patients with HIV/AIDS- An emerging clinicalproblem. Current Cardiology Reviews,2009;5:149-154
- Bonnet D. Cardiovascular complications in HIV infected children. BarraroG, Borraa F(editors): In Cardiovascular disease in AIDS, Springer-Verlag Italia 2009,2nd edition pp: 181-189
- PalellaF,PhairJP.Cardiovascular disease in HIV infection. Curr Opin HIV/AIDS 2011;6(4):266-271
- Lipshultz SE,Easley KA,Orav EJ, et al. Cardiac dysfunction and mortality in HIV infected children: The prospective P2C2 HIV Multicenter study. Circulation 2000;102(13): 1542-1548
- Syed FF,Sani MU. Recent advances in HIV-associated cardiovascular diseases in Africa. Heart 2013;99(16):1146-53
- Lumsden RH, Bloomfield GS.The causes of HIV-associated cardiomyopathy:A tale of two worlds.Biomed Research International 2016;2016:8196560.doi:10.1155/2016/8196560
- ThienemannF,SliwaK,Rockstroh JK.HIV and the heart: the impact of antiretroviral therapy: a global perspective. Eur Heart J.2013; 34(46):3538-46
- Bloomfield GS,BarasaFA,DollJA,Velazquez EJ. Heart failure in sub-Saharan Africa. Curr Cardiol Rev.2013;9(2):157-73
- TwagirumukizaM, NkeramihigoE, Seminega B, et al. Prevalence of dilated cardiomyopathy in HIV-infected African patients not receiving HAART: amulticenter, observational, pros pective, cohort study in Rwanda. Curr HIV Res 2007;5(1):129-37
- Manga PM.HIV and heart disease in Africa. J Am Coll Cardiol. 2015;66(5):586-8
- BadalS, GuptaR,KumarP ,Sharama M, Chhajta DS.Cardiac manifestations inHIV infected children. Are they under diagnosed? HIV/AIDS Res Treat Open J.2015;2(1):21-26
- NzuobontaneD, BlackettKN, Kuaban C. Cardiac involvement in HIV infected people inYaounde, Cameroon. Postgrad Med J 2002;78:678-681
- PongprotY, Sittiwangkul R, Silvilairat S, Sirisanthana V. Cardiac manifestations in HIV –infected Thai children. Annual of Tropical Pediatrics 2004(24):153-159
- SliwaK,CarringtonMJ,Becker A et al. Contribution of the human immunodeficiency virus/acquired immunodeficiency syndrome epidemic to de novo presentations of heart disease in the Heart of Soweto Study cohort. European Heart Journal, 2012(33):866-874
- Miller TL, Orav EJ, Lipshultz SE et al. Risk factors for cardiovascular disease in Human Immunodeficiency Virus-1 infected children. J Pediatr 2008;153(4):491-497
- Barbaro G.Cardiovascular manifestations of HIV infection. Circulation 2002;106: 1420-1425
- Chetlin M,Bartlett JG,Bloom A.Cardiac involvement in HIV infected patients.Up To Date, version 21.6,October 2010.
- Chen Y,WatsonRR. Causative factors of cardiovascular complications in AIDS. BarraroG,Borraa F(editors): In Cardiovascular disease in AIDS, Springer-Verlag Italia 2009,2nd edition pp:109-118
- Dworkin BM,Antonecchia PP,Smith F,et al. Reduced cardiac selenium content in the acquired immunodeficiency syndrome. JPEN J Paretral Nutr 1989;13(6):644-7
- Lewis W, Grupp IL, Grupp G, et al. Cardiac dysfunction occurs in the HIV-1 transgenic mouse treated with zidovudine. Lab Invest 2000; 80:187.
- Domanski MJ, Sloas MM, Follmann DA, et al. Effect of zidovudine and didanosine treatment on heart function in children infected with human immunodeficiency virus. J Pediatr 1995;127:137
- Longo-Mbenza B, SeghersKV, PhuatiM, BikangiFN, MubawaK. Heart involvement and HIV infection in African perspective: determi - nants of survival. Int J Cardiol 1998;64(1): 63-73
- LipshultzSE,EasleyKA, Orav EJ, et al. Left ventricular structure and function in children infected with human immunodeficiency virus :The prospective P2C2 HIV Multicenter study. Circulation 1998;97(13):1246-1256
- Starc TJ, Lipshultz SE,Kalpan S. Cardiac copmplications in children with Human immunodeficienct virus infection. Pediatrics, 1999;104(2):e14
- NetoMG, ZwirtesR, Brites C. A literature review on cardiovascular risk in human immunodeficiency virus-infected patients: implications for clinical management. Braz J Infec Dis 2013;17(6):691-700
- Fisher SD, Lipshutz SE. Cardiovascular abnormalities in HIV infected individuals .MannDL,ZippsDP,BonowRO,LibbyP,Braunw ald E (editors):In Brawnwald heart disease: A textbook of cardiovascular medicine,Elsevier Saunders,10th edition, 2015.PP:1624-1635
- Currier JS. Update on cardiovascular complica -tions in HIV infection. Topics in HIV Medicine,2009;17(3):98-103
- Patel K, Van Dyke RB, Mittleman MA et al. The impact of HAART on cardiomyopathy among children and adolescents perinatally infected with HIV-1. AIDS 2012;26:2027-2037
- Remick J,Geogiopoulou V, Mati C etal.Heart failure with human immunodeficiency virus infection:Epidemiology,pathophysiology,treatm ent and future research. Circulation; 129(17):1781-1789
- Lipsultz SE, Williams PL, Wilkinson JD et al. Cardiac status of HIV-infected children treated with long-term combination antiretroviral therapy: Results from the Adolescent Master Protocol of the NIH Multicenter Pediatric HIV/AIDS Cohort Study. JAMA Pediatr 2013;167(6):520-527
- Mondy KE, GottdienerJ,OvertonET,et al. High prevalence of echocardiographic abnormalities among HIV –infected persons in the era of highly active antiretroviral therapy.Clin Infec Diseases 2011;52(3):378-386
- Mast HI, Halter JO, Schiller MS, Anderson VM. Pericardial effusion and its relationship to cardiac disease in children with acquired immunodeficiency syndrome. Pediatr Radiol 1992;22:548-551
- BakariM, Chillop, LwakatareJ. Factors associated with, and echocardiographic findings of heart failure among HIV- infected patients at a tertiary health care facility in DareesSalaam, Tanzania. Tanzan J Health Res 2013;15(2): 73-81
- NtusiN,O’ DwerE, DorrelL, et al.HIV-1-Related cardiovascular disease is associated with chronic inflammation, frequent pericardial effusions,and probabale myocardial edema. Cir Cardiovasc Imaging 2016;9(3):e004430 doi:1 0.1161/CIRCIMA GING.115.004430
- RestrepoCS, DiethelmL LemosFA, etal. Car - diovascular complications of human immunodeficiency virus infection. Radio graphics 2006;26:213-231
- Reinsch A L, Neuhaus K,Esser S, et al. Pericardial effusion of HIV-infected patients-results of a prospective multicenter cohort study in the era of antiretroviral therapy. Eur J Med Res 2011;16: 480-483
- CegielskiJP,RamiiyaK,Lallinger GJ, Mtulia IA, Mbaga IM. Pericardial disease and human immunodeficiency virus in Dare esSalaam, Tanzania.Lancet 1990;335(868):209-12
- Chen y,Brenessel D,Walters J et al.Human immunodeficiency virus-associated pericardial effusion : report of 40 cases and review of the literature. Am Heart J1999;137:516
- Myosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis.Circulation 2005;112: 3608-3616
- Maher D,HarriesAD.Tuberculous pericardial effusion:a prospective clinical study in a low-resource setting-Blantyre,Malawi.Int J Tuberc Dis,1997;1(4):358-64
- Janda S, Quon BS, Swiston J. HIV and pulmonary arterial hypertension: a systematic review. HIV Medicine 2010;11:620-634
- Barbaro G. Cardiovascular manifestations of HIV infection. J R Soc Med 2001;94:384-390
- AlmodovarS,CicaliniS,PetrosilloN,Flores SC. Pulmonary hypertension associated with HIV infection. Pulmonary vascular disease: the global perspective. CHEST 2010;1 37(6)Suppl:6S-12S
- Binga JR,Sime PS,Koulla- shiro s.HIV related pulmonary arterial hypertension: Epidemiology in Africa,physiopathology and role of antiretroviral treatment. AIDS Research Therapy 2015;12(36):DOI 10.1186/s12981-015-0078.3
- PetitpretzP,BrenotF,Azarian R, et al. Pulmon - ary hypertension in patients with human immunodeficiency virus infection .Comparison with primary pulmonary hypertension. Circulation 1994;89:2722-2727
- Van Doorn CA M,Yates R, Tsang VT. Endocarditis as the first manifestation of AIDS in infancy. Arch Dis Child 1998;79:179-180
- CicaliniS,ForcinaG,DeRosaFG. Infective endocarditis in patients with human immunodeficiency virus infection.J Infec 2001;42(4):267-71
- NelSH,Naidoo DP. An echocardio cardiog - raphic study of infective endocarditis, with special reference to patients with HIV. Cardiovasc J Afr 2014;25(2):50-7
- Gebo KA, Burkey MD, Lucas GM, et al. Incidence of, risk factors for, clinical presentation, and 1-year outcomes of infective endocarditis in an urban HIV cohort. J Acquir Immune Defic Syndr 2006; 43:426
- Lipshultz SE, Chanock S, Sanders SP, et al.Cardiovascular manifestations of human immunodeficiency virus infection in infants and children.Am J Cardiol 1989;63:1489-1497
- Bharati S,Joshi VV,Conner EM et al.Conduction system in children acquire immunodeficiency syndrome.Chest 1989;98:406-413
- Tseng ZH,SecemskyEA, DowdyD, et al: Sudden cardiac death in patients with human immunodeficiency virus infection. J Am Coll Cardiol 2012; 59:1891-6
- OgunmolaOJ,OladosuYO,Olamoyegun MA. QTc interval prolongation in HIV- negative versus HIV-positive subjects with or without antiretroviral drugs. Ann Afr Med 2015;14(4): 169-76
- Nordin C, Kohli A, Beca S, et al: Importance of hepatitis C coinfection in the development of QT prolongation in HIV-infected patients. J Electrocardiol 39:199, 2006
- Triat VA.HIV infection and coronary heart disease: An intersection of epidemics.The Journal Infectious Diseases 2012;205:S355-61
- DAD Study Group: Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med 356:1723, 2007.
- Barlow-MoshaL,EckardAR, McComseyGA,MusokePM. Metabolic complications and treatment of perinatally HIV-infected children and adolescents. Journal of the International AIDS Society 2013;16:18600
- ReyskensKM,Fisher TL SchislerJC,et al. Cardio-metabolic effects of HIV proteaseinhibitors (lopinavir/ritonavir). Plos One,2013;30:8(9):e73347.doi:10.1371/journal. pone.007347.eCollection2013
- Rosmeri KL, Regina K, Eduardo S, et al: Clinical research: Dietary intervention prevents dyslipidemia associated with highly active antiretroviral therapy in human immunodeficiency virus type 1–infected individuals. A randomized trial. J Am Coll Cardiol 59:979, 2012.
- Dollfus C, Chenadec J L,FayeA,et al. Long-term outcomes in adolescents perinatally infected with HIV-1 and followed up since birth in the French perinatal Cohort(EPF/ANRS CO10). Clin Infec Diseases 2010;51(12):214-224
- Diógenes MA, Succi RC,MachadoDM,et al. Cardiac longitudinal study of children perin - atally exposed to Human immune odefici -ency virustype 1. Arquivo sBrasileiros deCardiologia 2005;85(4):330-8
- Miller R,KaskiJP,Hakim J et al.Cardiac disease in adolescents with delayed diagnosis of vertically acquired HIV infection.Clin Infec Dis 2013;56:576-582
- AL-Attar I,OrawEJ,ExilV,Vlach SA, Lipshultz S.Predictors of cardiac morbidity and related mortality in children with acquired immunode ficiency syndrome. J Am CollCardiol 2003;41: 1568-605
- TemuTM, KiruiN, WanjallaC, et al. Cardiovasc -ular health knowledge and preventive practices in people living with HIV in Kenya.BMC Infec Dis.2015;15:42 1.doi:10.1186/s12879-015-1157-8
- GrinspoonS,Grunfeld C, Kolter D et al. Executive summary state of the science conference: Initiative to decrease cardiovascular risk and increase quality of care for patients living with HIV/AIDS.Circulation 2008;118(2):198-210
- Bloomfield GS,KhazanieP,Morris A et al.HIV and noncommunicable cardiovascular and pulmonary diseases in low-and middle-income countries in the ART era: what we know and best directions for future research. J Acqir Immune Defic Syndr 2014;67(o1):S40-S53
- Mocumbi AO.Cardiac disease and HIV in Africa: A case for physical exercise.Open AIDS J,2015;9:62-65
- MielJ,GranaD,AlonsoGF,MatturriL.Cardiac involvement in acquired immunodeficiency syndrome-a review to push action.Clin. Cardiol 1998;21: 465-472
- BarbaroG, Fisher SD, PellicelliAM, Lipshultz SE. The expanding role of the cardiologist in the care of HIV infected patients. Heart 2001;86:365-367
- GoehlerA, NolteJ,NewmanA,et al. Clinical benefit and cost-effectiveness of cardiovascular disease screening in HIV-infected patients. . J Am Coll Cardiol 2011; 57:e1186