


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
The Association between Pulmonary Aspergillus infections and the Immune Status of HIV/AIDS Subjects with Respiratory Symptoms
Ofonime M. Ogba
Copyright : © 2016 M. Ogba O. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Fungal respiratory disease results in high mortality among the immunocompromissed, such as HIV/AIDS patients. An early diagnosis of invasive aspergillosis based on mycological evidence is difficult to establish.
Methods: HIV-positive subjects with respiratory symptoms were enrolled for the study. Subjects selection was based on HIV screening and the ability to produce sputum. A structured questionnaire was administered to all the subjects after obtaining their informed consent for demographic data. Ethical approval was obtained from the ethical research committee, UCTH, Calabar, Nigeria. Blood samples were obtained for CD4 count determination to ascertain the immune status of the patients. Sputum samples produced early in the morning were obtained twice from the subjects and subjected to macroscopy, microscopy and culture. The immune status of the subjects was assessed by CD4 count levels. Identification to the species complex level was performed by macroscopic and microscopic morphology.
Results: Aspergillus fumigatus was the most prevalent isolate (76.5%). Pulmonary aspergillosis (47.1%) occurred mostly in subjects aged 20 – 30 years. Mixed infections with other opportunistic respiratory pathogens occurred (1.5%) at CD4 counts levels lower than 200, but there was no statistically significant effect of co-infection on the immune status (H= 4.4, p = 0.22). HIV positive subjects with Aspergillus infections had lower mean CD4 counts (168.0±120.7) than those without this infection (354.4±255.7) (t = 2.97, p = 0.003).
Conclusion: Pulmonary aspergillosis is a public health challenge among HIV/AIDS patients in our locality. There was a strong association between CD4 count and pulmonary Aspergillus infection among HIV-seropositive patients. These infections seem to reduce CD4 counts. The CD4 count could be used alongside non culture methods for prompt and early diagnosis which is essential for effective patient management and a better patient outcome.
Keywords: Aspergillus infections; HIV/AIDS; pulmonary; CD4 counts.
1.Introduction
Exposure to Aspergillus infection is global but aspergillosis is uncommon unless drugs, other infections, or malignancy have altered the host immune defenses. Aspergillosis is a fungal infection which is life threatening among the immunocompromissed, especially human immunodeficiency virus (HIV) subjects [1].
Pulmonary aspergillosis is an opportunistic infection. Opportunistic infections (OIs) are main reason for diseased states and death among HIV/AIDS patients [2]. Data on the spectrum of pulmonary aspergillosis are not available in Calabar, Nigeria. Clinical and immunological profile of infected patients is scarce. This work generated data on these areas and is the first of its kind.
HIV status in the Locality: HIV/AIDS is a huge problem in Nigeria whose population is about 160 million. Nigeria is ranked third in the world in terms of the number of persons infected with HIV [3]. An estimated 3.3 million people were living with HIV/AIDS in 2010, with 281,180 new AIDS cases and 215,130 AIDS-related deaths. About 25% of tuberculosis cases occur in HIV positive patients (51/100,000) and 210/100,000 occur in the total population annually for HIV negative and HIV positive cases respectively [4]. Cross River State was reported to have the highest number of persons living with HIV in Nigeria. The infection levels rose from 4% to 12% between 1993 and 2003. However, the results of the sero-prevalence survey carried out in 2005 revealed a reduction from 12% to 6% [2].
Relationship between HIV and CD4 counts: The HIV usually infects CD4 T-lymphocyte cells. These cells are crucial elements of the immune system as they are involved in the fight against infections. The HIV infects these cells and reproduces copies of viruses. Immunosuppresion makes the patients liable to different respiratory syndromes including aspergillosis [5].
Acute invasive aspergillosis is a devastating opportunistic infection in the severely immunocompromissed. These diseases predominate in those with low CD4 cell counts (≤ 100/µl), non-suppressed HIV ribonucleic acid (RNA) levels, and among subjects not receiving antiretroviral therapy (ART) [6]. Invasive aspergillosis principally involves the Sino pulmonary tract via inhalation of Aspergillus spores. Symptoms of pulmonary aspergillosis are non-specific includes: fever, cough, and dyspnea [7].
The gold standard in the diagnosis of IPA is by the microscopic demonstration of fungal hyphae in histologically stained lung tissue obtained by open-lung biopsy or thoracoscopy. The diagnosis is difficult and involves a positive culture results from normally sterile samples (e.g., pleural fluid) [8]. This prospective cross-sectional study was designed to assess: the spectrum and prevalence of pulmonary Aspergillus infections among HIV positive subjects in our locality and to correlate the relationship between probable invasive pulmonary aspergillosis and CD4 count levels among these subjects.
2.Methods
Ethical approval was obtained from the ethical research committee, UCTH, Calabar, Nigeria. Subjects’ enrollment was based on HIV-positivity, complaints of respiratory symptoms and the ability to produce sputum. All adult subjects provided written informed consent for sampling in addition to providing consent for the structured questionnaire. Parents or guardian of children participant provided informed consent on their behalf. A structured questionnaire was administered to all the subjects for demographic data, after obtaining their informed consent.
Study population: Human immunodeficiency virus positive subjects of both gender numbering 272 with respiratory symptoms were enrolled for the study. The HIV positive subjects without respiratory symptoms and those who were on antifungal chemotherapy in the past three weeks were excluded from the study.
Sample collection: Convenient sampling method was used. Sputum samples produced early in the morning were obtained twice from the subjects and subjected to macroscopy, microscopy and fungal culture. Five mls of venous blood samples were obtained for CD4 count determination to ascertain the immune status of the patients. Identification to the species complex level was performed by macroscopic and microscopic morphology.
Data analysis: Epi Info 2010 statistical software was used to analyse the data. The summary of the continuous variables were presented as means and standard deviation using one sample t-test. Frequencies were calculated for categorical variables. Interactions between specific categorical clinical variables were tested for significance using the χ² test.
3.Results and Discussion
Positive cultures were confirmed in the second samples submitted by subjects. Three Aspergillus species were encountered among subjects. Aspergillus fumigatus was the most prevalent isolate (76.5%) among subjects (Figure. 1).
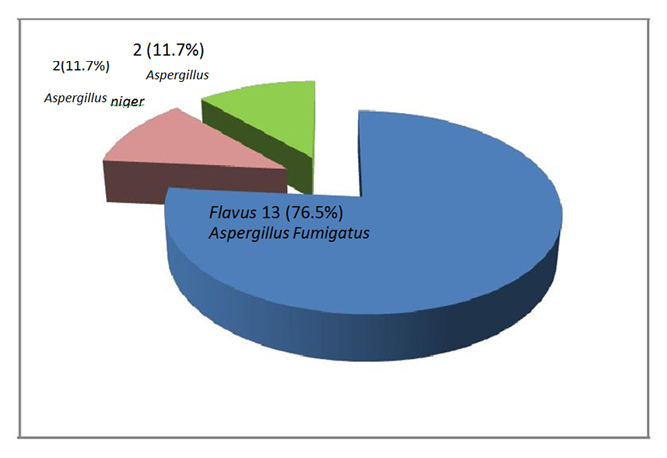
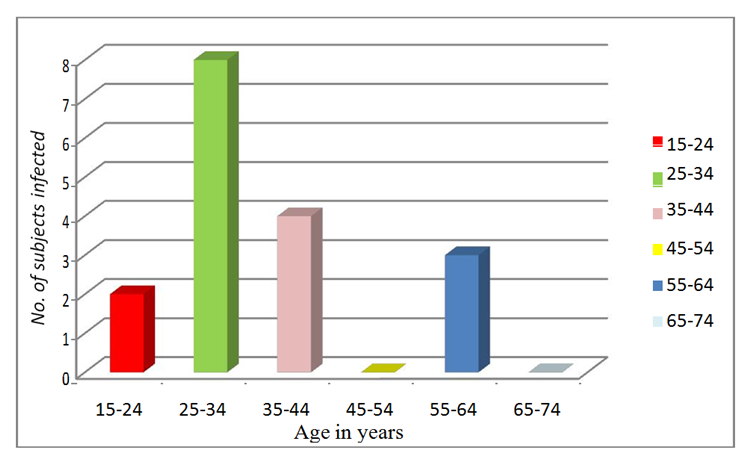
Figure 2 shows the distribution of Aspergillus infection among subjects by age. Pulmonary aspergillosis (47.1%) occurred mostly in subjects aged 20 to 30 years.
The most common presenting symptoms among subjects positive for aspergillus infections were cough (17/17, 100%) and chest pain (8/17, 47.0%); other symptoms include; fever (6/17, 35.2%), hemoptysis (5/17, 29.4%), weight loss (5/17, 29.4%) and sinusitis (2/17, 11.7%). There was a statistically significant relationship between presenting symptoms and type of Aspergillus isolates among subjects (χ2=106.3, p = 0.01) (Table 1).
Aspergillus fumigatus was the most prevalent species (76.4%) among subjects with mean CD4 Counts 173.8±131.9. All Aspergillus infection occurred at CD4 count lower than 200/µl of blood. There was a statistically significant effect of the immune status of subjects on Aspergillus infection rates (Kruskal-Walis H = 11.1, p = 0.01) (Table 2).
Subjects with pulmonary aspergillosis (6.3%) had lower mean CD4 counts (168±120.7) than those without the infection (354.4±255.7). There was a statistically significant association between the immune status of subjects and the infection rates ((t = 2.97, p = 0.003) (Table 3).
Mixed infections with other opportunistic respiratory pathogens occurred (1.5%) at CD4 counts levels lower than 200, but there was no statistically significant association between co-infection on the immune status (H= 4.4, p = 0.22) (Table 4).
4.Discussion
The diagnosis of pulmonary aspergillosis remains challenging, early diagnosis is carried out with a high index of suspicion. In this study our subjects did not undergo lung surgery but high suspicion index comprising the symptoms, microscopic demonstration of septate branching Aspergillus hyphae accompanied by a positive culture result in sputum collected twice from the subjects.
All the subjects presented with productive cough, this is different from the report of Denning et al [9] whose subjects presented more frequently with non-productive cough. Chest pain, hemoptysis and fever were the most presenting symptoms among subjects with Aspergillus fumigatus infection. Subjects with A. fumigatus infections were more symptomatic than other subjects which may indicate a more invasive nature of these fungi.
Aspergillus species infections have been associated with significant morbidity and mortality among immuno compromissed patients. In this study an infection rate of 6.3% was recorded among the subjects. This is lower than the 27.9% Aspergillus infection rate reported by Ochiabuto et al [10] in South Eastern Nigeria. The lower infection rates in our study could be due to the effectiveness of HAART therapy among the subjects as all subjects were enrolled from treatment centers.
Aspergillus fumigatus has been the most implicated in pulmonary infections. In this study, A. fumigatus accounted for 76.4% of the isolates followed by Aspergillus flavus and A. niger with 11.8% infection rates each. This is in agreement with the reports of Ochiabuto et al [10] in South Eastern Nigeria who also reported Aspergillus fumigatus as the most prevalent 41.2% species among their subjects. Patterson et al [11] also stated that Aspergillus fumigatus causes 60-90% invasive aspergillosis. On the other hand Bulpa et al [12] reported that 3.6% invasive pulmonary aspergillosis (IPA) were due to A. niger. Their report is lower than the 11.8% prevalence in this study which may have been due to the depressed immune status of the subjects.
The mean age of subjects with infection was 28.4± 16.8, with 70.6% in their second and third decade of life. Subjects in this age group were more infected probably because of their high sexual activity which may have resulted in high HIV transmission rates and the resulting opportunistic infections. On the other hand, subjects in this age bracket are also economically productive, therefore morbidity and mortality amongst them results in loss of man hours which affects their household and the Nation.
Holding and colleagues [13] reported the association of aspergillosis with CD4 lymphocytopenia among people with HIV infection. In this study all Aspergillus infection occurred at CD4 count lower than 200cells/µl of blood. There was a statistically significant effect of the immune status of subjects on Aspergillus infection rates (Kruskal-Walis H = 11.1, p = 0.01).
In the present study 17(6.3%) subjects with pulmonary aspergillosis were associated with mean CD4 cells of 168.0±120.7 cells/µl of blood. This is in agreement with the reports of Khan et al [14] who stated that when the CD4 count is below 150/mm3, fungal infections such as Aspergillosis should be considered invasive.
5.Limitations of Study
Radiological diagnosis were not carried out which could have led to a more specific diagnosis. We did not carry out patients follow up for final patient’s outcome. This could have revealed the mortality rate amongst our subjects.
6.Conclusion
There was a strong association between CD4 count and pulmonary Aspergillus infection among HIV-seropositive patients. The CD4 count could be used alongside non culture methods for prompt and early diagnosis which is essential for effective patient management and a better patient outcome. Further research is needed to understand if other immune defects such as impaired cytokine production, are associated with pulmonary aspergillosis.
7.Acknowledgement
We are grateful to the management and staff of UCTH and Lawrence Henshaw Hospital for the use of their subjects and facilities and University of Calabar for the enabling environment for research.
8.Author’s Summary
Pulmonary aspergillosis is an opportunistic infection (OI). It is a devastating opportunistic infection in the severely immunocompromissed. Nigeria is ranked third in the world in terms of the number of persons infected with HIV and as such immunosuppressed with OIs. Data on the spectrum of pulmonary aspergillosis are not available in Calabar, Nigeria. Clinical and immunological profile of infected patients is scarce. This work generated data on these areas and is the first of its kind. In this study an infection rate of 6.3% was recorded among the subjects. The infections were associated with mean CD4 counts of 168.0±120.7 cells/µl of blood. The CD4 count could be used alongside non culture methods for prompt and early diagnosis. Further research is needed to understand if other immune defects such as impaired cytokine production are associated with pulmonary aspergillosis.
References
- Walsh TJ., Anaissie EJ., Denning D. W. (2008). Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis 2008; 46:327–60.
- Ogba, OM., Abia-Bassey LN & Epoke J. (2013). The relationship between opportunistic pulmonary fungal infections and CD4 count levels among HIV-seropositive patients in Calabar, Nigeria. Transactions of the Royal Society of Tropical Medicine and Hygiene January 2013; 107(3): 170-5. doi: 10.1093/trstmh/trs025.
- Federal Ministry of Health. National guidelines for HIV and AIDS treatment and care in adolescents and adults 2007; Abuja: FMH Press.
- WHO progress report 2011. http://www.who.int/HIV/pub/progress_report 2011/en/index.html
- International Association of Providers of AIDS Care. The AIDS InfoNet 2014; Factsheet 500.
- Marukutira T, Huprikar S, Azie N et al. Clinical characteristics and outcomes in 303 HIV-infected patients with invasive fungal infections: data from the Prospective Antifungal Therapy Alliance registry, a multicenter, observational study. HIV AIDS (Auckl) 2014; 6:39–47.
- Nash G, Irvine R, Kerschmann RL, Herndier B. (1997). Pulmonary aspergillosis in acquired immune deficiency syndrome: autopsy study of an emerging pulmonary complication of human immunodeficiency virus infection. Hum Pathol 1997; 28:1268–1275.
- Horii KA, Nopper AJ. Emerging cutaneous infections in the premature neonate. Adv Dermatol. 2007; 23:177–195.
- Denning DW, Follansbee SE, Scolaro M, Norris S, Edelstein H, Stevens DA. “Pulmonary aspergillosis in the acquired immunodeficiency syndrome,” The New England Journal of Medicine 1991; 324(10): 654–662.
- Ochiabuto OMT, Nwankwo A, Enweani IB, Okoye JO, Okeke CO, Nwankwo M, Nwafuluaku MI and Obi CM. Fungal Isolation in HIV Patients and CD4 Count. International STD Research & Reviews 2014; 2(2): 101-112, 2014; Article no. ISRR.2014.2.006
- Patterson, T. F., Kirkpatrick, W. R., White, M., Hiemenz, J. W., Wingard, J. R., Dupont, B., Rinaldi, M. G., Stevens, D. A. & Graybill, J. R. for the Aspergillus Study Group (2000). Invasive aspergillosis: disease spectrum, treatment practices, and outcomes. Medicine (Baltimore) 79: 250–260.
- Bulpa, P., Dive, A. & Sibille, Y. Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. Eur Respir J. 2007; 30, 782–800.
- Holding, KJ., Dworkin, MS., Wan, PT., Hanson, DL., Klevens, RM., Jones, JL., Patrick S. & Sullivan PS. Aspergillosis among People Infected with Human Immunodeficiency Virus: Incidence and Survival. Clinical Infectious Diseases 2000; 31: 1253-1257.
- Khan PA, Malik A, Fatima N, Shameem M. Profile of Fungal Lower Respiratory Tract Infections and CD4 Counts in HIV Positive Patients. Virol. Mycol 2013; 2: 113. doi:10.4172/2161-0517.1000113