


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Dermatology
Volume-1 Issue-3, 2016, Page No: 14-16
Interstitial Granulomatous Dermatitis Induced by Simvastatin
Rosa Gimenez-Garcia, Eva Martinez Martin
Hospital Rio Hortega, Valladolid, Spain.
Citation : Garcia RG, Martin EM. Interstitial Granulomatous Dermatitis Induced by Simvastatin. ARC Journal of Dermatology. 2016;1(3):14–16.
Copyright : © 2016 Garcia RG. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Reactive granulomatous dermatitis represent cutaneous reactions pattern that occur in the setting of a systemic trigger, including connective tissue diseases, arthritis, malignancy and drugs. We report a case in which an IGDR triggered by simvastatin.
Case Report: A 68-year-old woman, with dyslipidaemia, presented with a 6 months history of skin lesions that developed after starting treatment with simvastatin. Physical examination revealed the presence of bilateral and symmetrically distributed erythematous plaques over her thighs. Histopathological findings from skin biopsy showed an interstitial predominantly lymphocytic infiltrate with mall granulomas including rare giant cells surrounding foci of collagen fragmentation. These findings were characteristic for an interstitial granulomatous drug reaction. Skin lesions resolved after discontinuation of simvastatin.
Discussion: Drug-induced interstitial granulomatous dermatitis was first described in 1998. In this initial description, calcium channel blockers, β-blockers, lipid-lowering agents and angiotensin –converting enzyme inhibitors were the most common offending agents. The list of culprit drugs has increased with time and include also antihistamines, diuretics, antidepressants, allopurinol, thalidomide, anti-TNF αagents, febuxostat, gabapentine, ganciclovir, Chinese herb extract, sorafenib, adalimumab, anakinra, darifenacinand soy. IGDR is probably underdiagnosed because of the variability of its cutaneous expression and a definitive diagnosis requires histological examination. The etiopathogenesis of reactive granulomatous dermatitis is unclear.
Conclusions: Patients with interstitial granulomatous dermatitis should be evaluated for underlying autoimmune disease, malignancy or drug reaction and should be closely followed up.
1.Introduction
Statins, or 3-hydroxy-3-methyl-glutaryl coenzyme-A (HMG-CoA) reductase inhibitors, are among the most prescribed drugs internationally. These drugs have proved clinical benefits in hypercholesterolemia and in the primary and secondary prevention of cardiovascular and cerebrovascular events [1-3].
Statins in general have a favourable safety profile, however, several and serious systemic and dermatological side effects have been registered, such as myopathy, diabetes mellitus, hepatotoxicity, autoimmune reactions and eosinophilic fasciitis. Diverse dermatological reactions include urticaria, eczema, dermatitis, lichenoid eruptions, pemphigus erythematosus, subacute cutaneous lupus erythematosus dermatomyositis, porphyria cutanea tarda, phototoxicity, cheilitis, generalized exanthematous pustulosis, chronic actinic dermatitis, occupational contact dermatitis, bullous dermatosis and toxic epidermal necrolysis [4].
Reactive granulomatous dermatitis represent cutaneous reactions pattern that occur in the setting of a systemic trigger, including connective tissue diseases, arthritides, malignancy and drugs [5]. Interstitial granulomatous drug eruption (IGDR), is a drug induced skin disease [5-7]. We report a case triggered by simvastatin.
2.Case Report
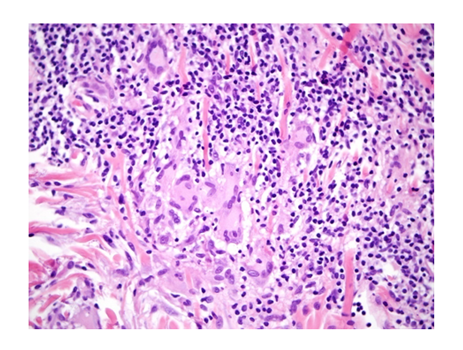
A 68-year-old woman, with personal history of allergy to nonsteroidal anti-inflammatory drugs and dyslipidaemia, presented with a 6 months history of skin lesions that developed after starting treatment with simvastatin and increase of transaminases. Physical examination revealed the presence of bilateral and symmetrically distributed erythematous plaques over her thighs (Figure 1). Histopathological findings from skin biopsy showed an interstitial predominantly lymphocytic infiltrate with small granulomas including rare giant cells surrounding foci of collagen fragmentation. (Figure 2) These findings were characteristic for an interstitial granulomatous drug reaction. Skin lesions resolved after discontinuation of simvastatin.
Figure 1
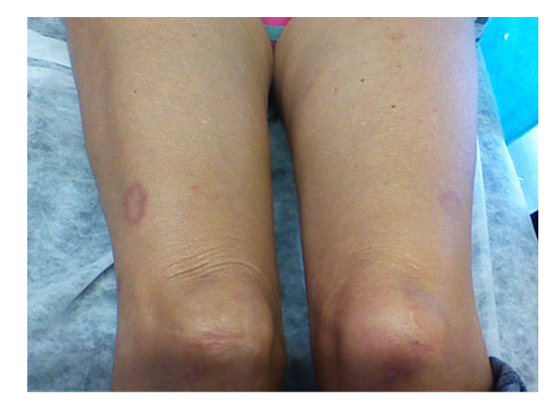
Figure 2
3.Discussion
Interstitial granulomatous dermatitis, first described in 1993 by Ackerman, is a distinct histopathological pattern seen in association with various systemic diseases, mostlyrheumatologic, neoplastic, or drug adverse reactions. Histology demonstrate interstitial granulomatous infiltrate surrounding foci of degenerated collagen in the reticular dermis [8, 9].
Clinical features include linear subcutaneous cords or bands (the rope sign), erythematous to violaceous papules or plaques with annular or polycyclic morphology, most commonly located symmetrically on the lateral aspects of the trunk, groin, buttocks and proximal limbs [4, 9]. Differential diagnosis include granuloma anular, necrobiosis lipoidica ormycosis fungoide [10].
Drug-induced interstitial granulomatous dermatitis, first reported by Magro et al.in 1998 [11]. In this initial description, calcium channel blockers, β-blockers, lipid-lowering agents and angiotensin –converting enzyme inhibitors were the most common offending agents. The list of culprit drugs has increased with time and includes also antihistamines, diuretics, antidepressants, allopurinol, thalidomide, anti-TNF α agents, febuxostat, gabapentine, ganciclovir, Chinese herb extract, sorafenib, adalimumab, anakinra, darifenacin and soy [12]. The etiopathogenesis of reactive granulomatous dermatitis is unclear. The diagnosis is challenging because of the prolonged time between the initiation (average 5 years) and cessation of the culprit drug and the emergence and clearance of lesion [12]. IGDR is probably underdiagnosed because of the variability of its cutaneous expression and a definitive diagnosis requires histological examination. The condition is treated by identifying and discontinuing the drug causing the reaction.
Patients with interstitial granulomatous dermatitis should be evaluated for underlying autoimmune disease, malignancy or drug reaction and should be closely followed up.
References
- Miller PE, Martin SS. Approach to statin use in 2016: an Update. Curr Atheroscler Rep 2016; 18:20.
- Thai SA, Reeve E, Hilmer SN, Qi K, Pearson SA, Gnjidic D. Prevalence of statin-drug interactions in older people. Eur J Clin Pharmacol 2016; 72:513-21.
- Beckett RD, Schepers SM, Gordon SK. Risk of new-onset diabetes associated with statin use. SAGE Open Med. 2015 Sep 30; 3: 2050312115605518.
- Jowkar F, Namazi MR. Statins in dermatology. Int J Dermatol. 2010;49 (11):1235-1243.
- Rosenbach M, English JC. Reactive granulomatous dermatitis. A review of palisade neutrophilic and granulomatous dermatitis, interstitial granulomatous dermatitis, interstitial granulomatous drug reaction and proposed reclassification. Dermatol Clin 2015; 33:373.387.
- Dodiuk-gad RP, Shear NH. Granulomatous drug eruptions. Dermatol Clin 2015; 33: 525-39.
- Perrin Ch, Lacour JP, Castanet J, Michiels JF. Interstitial granulomatous drug reaction with a histological pattern of interstitial granulomatous dermatitis. Am J dermatopathol 2001; 23: 295-8.
- Blazewicck I, Szczerkowska-Dobosz A, Peksa R, Stawczyk-Macieja M, Baranska-Rybak W, Nowicki R. Interstitial granulomatous dermatitis: a characteristic histological pattern with variable clinical manifestations. Postepy Dermatologii Alergologii 2015; 6: 475-477.
- Coutinho I, Pereira N, Gouveia M, Cardoso JC, Tellechea O. Interstitial granulomatous dermatitis. Am J Dermatopathol 2015; 37: 614-9.
- Debarbieux S, Balme B, Thomas l. Dermatite interstitielle granulomateuse. Ann Dermatol Venereol 2007; 134: 889-891.
- Magro CM, Crowson AN, Schapiro BL, . The interstitial granulomatous drug eruption a distinctive clinical and pathological entity. J Cutsn Pathol 1998; 25:72-8.
- Dodiuk-Gad RP, Shear NH. Granulomatous drug eruptions. Dermatol Clin 2015; 33: 525-39.