


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
ARC Journal of Clinical Case Reports
Volume-2 Issue-1, 2016, Page No: 5-8
Acute Cardio respiratory Decompensation in a Child with Nephrotic Syndrome with Bronchial Asthma: is it Exaggeration of Bronchial Asthma?
Tomar Munesh, MD, FNB 1, Azad Sushil MD, FNB 1, Sethi Siddharth, MD 2
1.Department of Pediatric Cardiology and Congenital Heart disease, Medanta-The Medicity, Gurgaon,India.
2.Department of Nephrology, Medanta-The Medicity, Gurgaon, India.
2.Department of Nephrology, Medanta-The Medicity, Gurgaon, India.
Citation : Tomar M, Azad S, Sethi S. Acute Cardio respiratory Decompensation in a Child with Nephrotic Syndrome with Bronchial Asthma: is it Exaggeration of Bronchial Asthma? ARC Journal of Clinical Case Reports. 2016;2(1):5–8.DOI : dx.doi.org/10.20431/2455-9806.0201002
Copyright : © 2016 Tomar M. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Patients with Nephrotic syndrome have increased tendency for thromboembolism . Pulmonary thrombo-embolism is life threatening complication. We report a case of 3 yrs old patient a known case of Nephrotic syndrome with bronchial asthma who presented with severe respiratory distress requiring ventilatory support .He was diagnosed with massive bilateral pulmonary embolism and treated successfully with thrombolysis.
Keywords: Nephrotic Syndrome, Pulmonary Embolism.
Abbreviations: Ao-Aorta,LPA-Left Pulmonary Artery,RPA-Right Pulmonary Artery,MPA-Main Pulmonary Artery.
1.Introduction
Thromboembolic episodes are one of the most serious complications in patients with nephrotic syndrome, with an overall incidence of 25%. Thrombosis in both the arterial and venous sides of circulation has been reported. This risk varies with the nature of the underlying disease and seems to be greatest for membranous nephropathy. Other factors, including the level of serum albumin, previous thromboembolic episodes, and a genetically determined predisposition to thrombosis, may also be involved. Pulmonary embolism if occurs can be life threatening if not diagnosed and treated on time. We report a case of 3 yrs old child a known case of Nephrotic syndrome who presented with this complication.
2.Case Report
A 3 yrs old male child, a known case of Nephrotic syndrome (frequent relapsing, failed on Levamisole ) and hyperreactive airway disease, presented in emergency with sudden onset respiratory distress. In view of his clinical condition he was immediately ventilated .As there was previous history of hyperreactive airway disease, 1st possibility for acute deterioration was thought of acute exacerbation of bronchial asthma. Arterial blood gas analysis showed severe metabolic acidosis (PH 7.2, PCO2 -43, PO2 78). His kidney function test showed creatinine = 0.8 mg/dl, urea = 62 mg/dl, Na = 122 mmol/l, K = 5.3 mmol/l, and urinalysis showed protein 3+. Other laboratory tests showed Hgb = 10.8 g/dl, serum albumin = 1gm/dl, total protein = 3.6 g/dl. As clinical and ABG parameters did not improve,cardiology opinion was taken. Twelve leads Electrocardiogram revealed sinus tachycardia and right heart strain pattern (Figure 1). With suspicion of pulmonary embolism, echocardiogram (Echo) was done which revealed dilated right atrium and right ventricle (RV), elevated RV pressures (mild tricuspid regurgitation with peak gradient of 70mmHg), flow in left pulmonary artery was not seen ? Complete occlusion of left pulmonary artery (LPA) by thrombus and right ventricular dysfunction. Computed tomography pulmonary angiography was done which confirmed the presence of thrombus in LPA along with occlusion right lower lobe branch of pulmonary artery(Qanadli score 28/40;left 20/20,right 8/20) (Figure2) .With diagnosis of acute pulmonary thromboembolism, immediate thrombolysis was started with tissue plasminogen activator ( t-PA) (dose 0.1 mg/kg/hr) . Repeat CT pulmonary angiography after 12 hrs of t-PA infusion did not reveal any significant change in LPA flow but right pulmonary artery branch opened completely. Child ventilator requirement also came down .Repeat echocardiography showed improvement in right ventricular function,reduction in pulmonary artery pressure (TR gradient 50 mmHg) but still there was no flow in left pulmonary artery. Repeat thrombolysis was started with higher dose (0.2 mg/kh/hour intravenous infusion ) but child had bleeding from central venous line site and because of bleeding thrombolysis was stopped. When bleeding stopped,child was started on heparin infusion .Repeat Echocardiography after 24 hours revealed further reduction in RV pressures (TR gradient 40 mmHg) and some flow into LPA was visualized . His clinical condition also improved and was extubated after 4 days. He was started on oral anticoagulants overlapped with intravenous heparin.
He was subsequently discharged after 15 days on oral anticoagulation (to maintain INR =2.5). Immediate follow up after 2 weeks revealed normal flow in LPA with normal RV pressures and function (Figure 3). CT pulmonary angiography repeated 3 months later revealed normal flow in both pulmonary arteries (Figure 4).
Figure1. 12 lead ECG showing sinus tachycardia, deep ‘S’ wave in lead I ‘T’ wave inversion in V1 and V2,right bundle branch block and low amplitude deflections
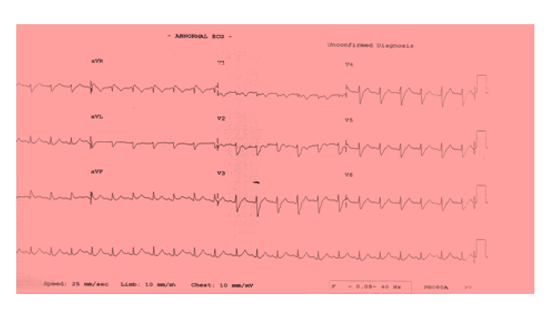
Figure2. CT pulmonary angiogram showing complete occlusion of left pulmonary artery with thrombus seen in lower lobe branch of right pulmonary artery(arrows)
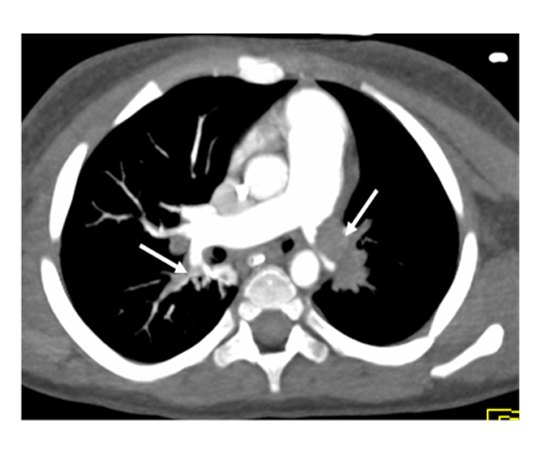
Figure3. Echocardiography with Color Flow Mapping Showing Normal Flow in Both Pulmonary Arteries
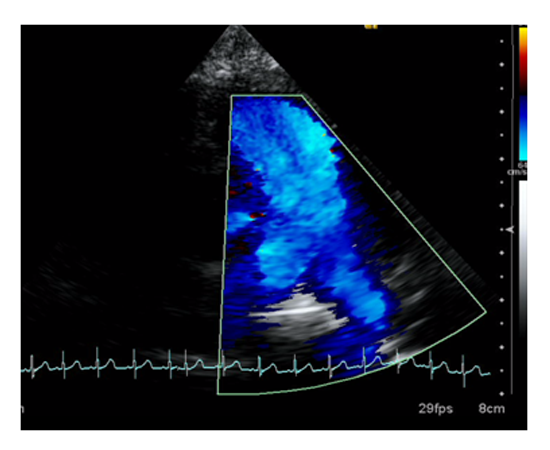
Figure4. CT Pulmonary Angiogram Showing Normal Flow in Both Right and Left Pulmonary Artery

3. Discussion
Patients with nephrotic syndrome are at increased risk of thromboembolic complications .The most frequent site of thrombosis is the deep vein and renal vein (1,2). Incidence of Arterial thromboses though less common than venous thromboses but occurs with higher frequency then general population(3). The pulmonary embolism(PE) is seldom reported in children, and many pulmonary embolism remain undiagnosed until postmortem examinations are performed. In a retrospective analysis of about 3600 autopsies performed during 25 years, Buck and his colleagues reported that the incidence of PE was 3.7% in the pediatric population (4). Bergquist pointed out that the mortality of the children with PE was 30% in cases with delayed diagnosis and treatment (5).
PE is a pathophysiological syndrome of pulmonary circulation disturbance due to lung vascular obstruction by endogenous and exogenous embolus or local thrombus. If hemorrhage and necrosis are present, pulmonary infarction is diagnosed. The occurrence of PE is related to sludge of blood flow, hypercoagulable status and impaired endothelial cells. Underlying mechanism for increased risk could be the result of impaired thrombolytic activity, imbalance between prothrombotic and antithrombotic factors, hypovolemia. Thromboembolic complications in nephrotic syndrome take account of increased coagulation factors VIII and fibrinogen, increased platelet adhesiveness, reduced anticoagulation factors such as antithrombin III, protein C and protein S levels and their activity, decreasing pro-fibrinolysin, increasing platelet counts, aggregation, attachment and releasing platelet alpha granules, with therapy of diuretics and corticosteroid (2,6).
The clinical presentations of PE are related to the speed of PE developing, the degree of vascular obstruction, the liberated vasoactive amines and the primary cardiopulmonary function status. The vascular obstruction is the most important factor. In the situation of small range of obstruction, few cardiodynamic and pulmonary functional changes are accompanied. An increased pulmonary artery pressure would not happen until 60% pulmonary vascular bed is occluded. Cyanosis and dyspnea generally occur when there is 65% obstruction. Severe pulmonary hypertension and shock will occur at 70%-80% obstruction, and death occurs at greater than 85% occlusion (7). It should always be suspected in any patient with Nephrotic syndrome presenting with respiratory distress. The use of V/Q scanning to screen asymptomatic children with nephrotic syndrome has demonstrated changes consistent with PE in 27.9 – 40% (8,9).
Thrombolysis is an established treatment for adults with PE associated with haemodynamic instability (10). No clear guidelines exist for the use of thrombolytic therapy in children with PE. Major complication of systemic thrombolysis is bleeding quoted at 37% (11). The indication for thrombolysis is most frequently cardiorespiratory distress or collapse, suggesting a poor risk group may account for the higher rate of major bleeding.
4.Conclusion
Children with nephrotic syndrome and very low serum albumin are at very high risk for thromboembolism . A high index of suspicion is needed by the physician as many of these thrombi are asymptomatic at presentation but can lead to potentially life-threatening complications. In stage of acute deterioration in these patients, pulmonary embolism should be suspected and managed aggressively.Pulmonary embolism carries very high mortality if not treated on time.
References
- Llach F.Hypercoagulability, renal vein thrombosis, and other thrombotic complications of Nephrotic syndrom . Kidney Int. 1985;28 (3):429
- Singhal R, Brimble KS.Thromboembolic complications of Nephrotic syndrome: Pathophysiology and clinical management. Thromb Res 2006;118:397
- Mahmoodi BK, Ten Kate MK, Waanders F et al .High absolute risk and predictors of venous and arterial thromboembolic events in patients with nephritic syndrome: results from large retrospective cohart study. Circulation 2008;117:224.
- Buck JR, Connors RH, Coon WW. Pulmonary embolism in children. J Pediatr Surg 1981;16:385-391.
- Bergquist D, Lindblad B. A 30-year survey of pulmonary embolism verified at autopsy: an analysis of 1274 surgical patients. Br J Surg 1985;72:105-108.
- Cameron JS. Coagulation and thromboembolic complications in the nephritic syndrome. Adv Nephrol Necker Hosp 1984;13:75-114.
- Evans DA, Wilmott RW. Pulmonary embolism in children. Pediatr Clin North Am 1994;41:569-584.
- Hoyer, P.F., Gonda, S., Barthels, M., Krohn, H.P. & Brodehl, J. (1986) Thromboembolic complications in children with nephrotic syndrome. Acta Paediatrica Scandinavica, 75, 804–810
- Huang, J., Yang, J. & Ding, J. (2000) Pulmonary embolism associated with nephrotic syndrome in children: a preliminary report of 8 cases. Chinese Medical Journal, 113, 251–253.
- Buller, H.R., Agnelli, G., Hull, R.D., Hyers, T.M., Prins, M.H. & Raskob, G.E. (2004) Antithrombotic therapy for venous thromboembolic disease: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest, 126, 401S–428S
- Gupta, A.A., Leaker, M., Andrew, M., Massicotte, P., Liu, L., Benson, L.N. & McCrindle, B.W. (2001) Safety and outcomes of thrombolysis with tissue plasminogen activator for treatment of intravascular thrombosis in children. Journal of Pediatrics, 139, 682–688.